





Perimenopause Symptoms or Nutrient Deficiencies? 10 Common Signs That Are Often Not Ovarian Decline
Perimenopause is a hormonal transition, not a catch-all explanation for feeling unwell. That matters because there is a trend right now where women compare symptoms online, label themselves perimenopausal, and feel confident purely because the symptom lists match.
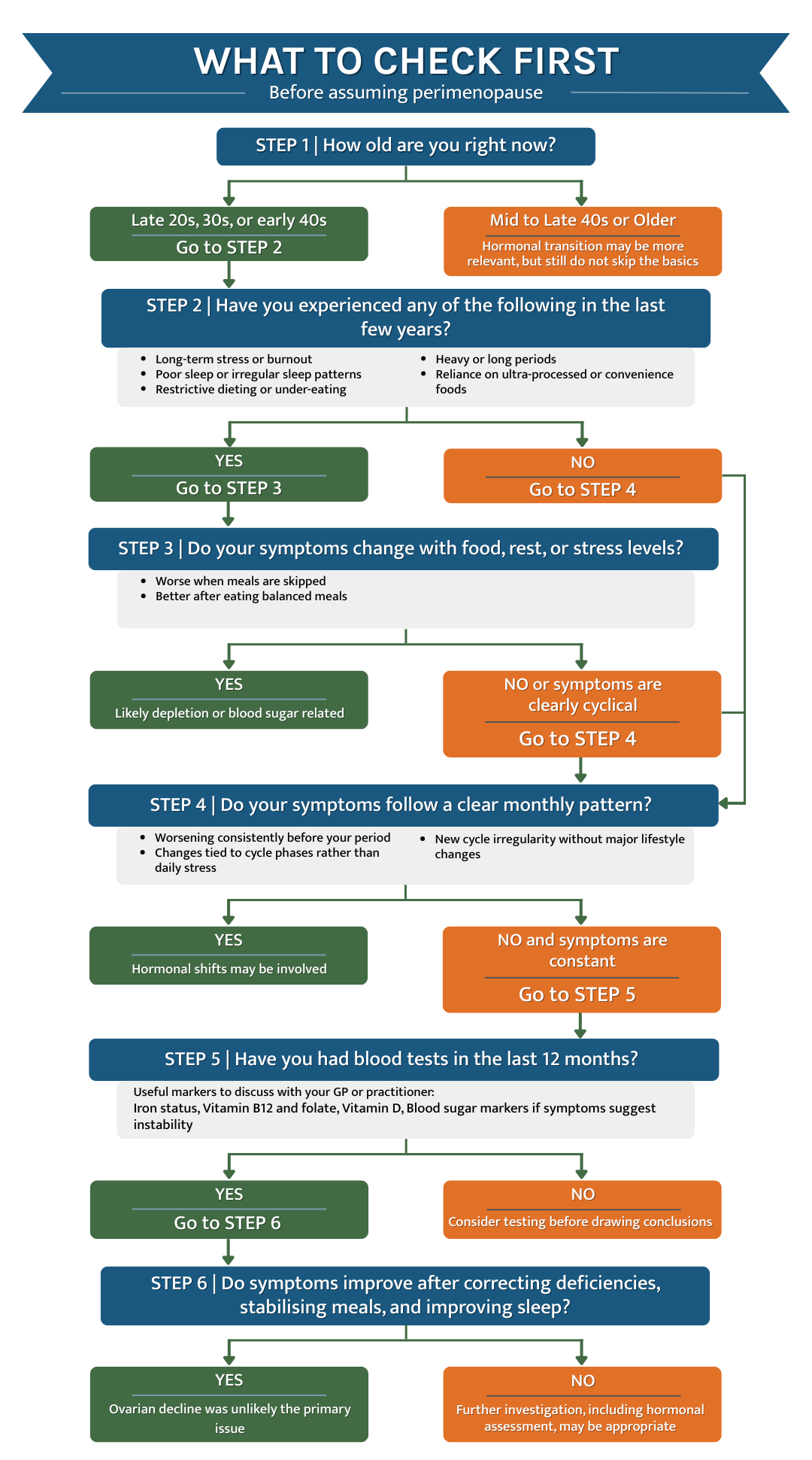
Symptoms matching a trend does not automatically mean ovarian decline. If you are in your late 20s, 30s, or early 40s, basic causes like nutrient depletion, blood sugar instability, stress, and poor sleep are often more likely than perimenopause.
This blog post is written to reduce confusion, not to dismiss you. Would you rather guess based on social media, or get clear and fix what is fixable first?
A quick scope note before we begin
This article assumes you are not on medication and you do not have diagnosed conditions such as diabetes, high blood pressure, or untreated thyroid disorders. That is important because medication side effects and chronic conditions can mimic many symptoms and require a different medical conversation.
Why symptom overlap is so common right now
Symptom overlap is common because the body has limited ways to signal strain. Fatigue, anxiety, poor sleep, brain fog, hair changes, and weight gain can come from hormones, but they can also come from depletion, under-fuelling, and unstable blood sugar.
Nutrient status influences energy production, cognition, mood regulation, and muscle function. Reviews show that multiple vitamins and minerals play measurable roles in fatigue and cognitive performance (Tardy et al., 2020).
So the question becomes simple. What if the problem is not a life stage, but a body that has been running on empty?
Symptoms that look like perimenopause but are often deficiencies
1. Fatigue and low energy
Fatigue is often the first symptom women label as perimenopause. Iron status can strongly influence physical and neuropsychological performance, especially in premenopausal women (McClung and Murray-Kolb, 2013).
Low micronutrient status is also linked to tiredness and reduced cognitive capacity. A broad evidence review links vitamin and mineral status with fatigue and energy metabolism (Tardy et al., 2020).
Clue it may not be perimenopause: fatigue improves within weeks once sleep, protein, and deficiencies are addressed.
2. Brain fog and poor concentration
Brain fog can feel hormonal because it is frightening and unfamiliar. Vitamin B12 plays a key role in neurological function, and deficiency can present with cognitive symptoms even before severe anaemia develops (O’Leary and Samman, 2010).
Iron status is also linked to attention and mental performance in women, particularly when iron stores are low (McClung and Murray-Kolb, 2013).
Clue it may not be perimenopause: symptoms worsen between meals or lift after a balanced meal.
3. Anxiety, low mood, or emotional volatility
Mood swings are commonly labelled perimenopause because that is what the algorithm suggests. Vitamin B6 supports neurotransmitter metabolism and has central roles in physiology that affect mood and neurological function (Parra et al., 2018).
Magnesium is also fundamental to neuromuscular and nervous system function. A major review outlines magnesium’s broad implications for health and disease, including pathways relevant to stress regulation (de Baaij, Hoenderop and Bindels, 2015).
Clue it may not be perimenopause: mood symptoms fluctuate daily and track stress, caffeine, or missed meals more than cycle timing.

4. Sleep problems and night waking
Sleep issues are often blamed on perimenopause even without hot flushes. Magnesium status has been associated with sleep quality in observational research, with systematic review evidence noting links between magnesium status and sleep patterns (Arab et al., 2023).
Clue it may not be perimenopause: you wake frequently at 2–4 am without night sweats, especially after late sugar or alcohol.
5. Hair thinning or hair loss
Hair loss is one of the easiest symptoms to mislabel as hormonal. Nutritional status is frequently discussed in the hair loss literature, including iron and other micronutrients (Tardy et al., 2020).
Zinc is often blamed online, but evidence is more nuanced than social media claims. A large cross-sectional study found slightly lower zinc levels among people with hair loss complaints, but the difference was minor and the authors did not recommend routine zinc testing for hair loss evaluation (Liran et al., 2025).
Clue it may not be perimenopause: shedding follows stress, illness, dieting, or low protein intake more than cycle changes.
6. Weight gain or difficulty losing weight
Weight changes are often attributed to “menopause metabolism” even in early 30s. Diet quality and carbohydrate type influence blood sugar regulation and metabolic health, which can drive cravings, fatigue, and weight gain patterns (Ludwig, Ebbeling and Holt, 2018).
Clue it may not be perimenopause: central weight gain pairs with energy crashes and strong cravings, especially mid-afternoon or late evening.
7. Irregular periods or heavier bleeding
This one is tricky because it can be perimenopause. Heavy bleeding can also drive iron depletion, which then worsens fatigue, palpitations, and weakness, creating a feedback loop (McClung and Murray-Kolb, 2013).
Clue it may not be perimenopause: cycles improve once iron status, stress, and fuelling are addressed.
8. Joint pain and muscle aches
Joint pain gets blamed on hormonal decline, but vitamin D status matters for muscle function and strength. A review on vitamin D and muscle function summarises mechanisms and clinical associations between low vitamin D and impaired muscle performance (Pfeifer et al., 2002).
Clue it may not be perimenopause: aches improve alongside vitamin D support, hydration, and recovery.
9. Palpitations or feeling wired but tired
Palpitations can feel like anxiety, and anxiety can feel hormonal. Iron deficiency anaemia is associated with symptoms including fatigue and palpitations, and psychiatric-type symptoms can overlap as well (Arshad et al., 2023).
Clue it may not be perimenopause: palpitations track low iron symptoms, stress surges, caffeine, or blood sugar dips.
10. Feeling not like yourself
Feeling unlike yourself is the most dangerous symptom to mislabel. Chronic depletion, poor sleep, and prolonged stress can change cognition, emotional stability, and resilience without any ovarian decline being the primary driver (Tardy et al., 2020).
Clue it may not be perimenopause: there is no clear cycle pattern, only constant depletion and reduced recovery.
What to do next if you want real clarity
Blood tests are the fastest way to replace guessing with evidence. If you want clear answers, speak to your GP or a qualified practitioner about a blood test that includes key markers relevant to your symptoms.
Ask yourself one direct question first. Have you actually checked your levels, or have you been trying to self-diagnose through content?
Suggested blog posts
Frequently Asked Questions
How can I tell if it is perimenopause or a nutrient deficiency?
The most practical distinction is pattern and response.
Perimenopause symptoms tend to follow hormonal shifts over time, while deficiency-related symptoms are often constant or fluctuate with food, sleep, stress, and recovery.
If symptoms improve noticeably after addressing nutrition, stabilising blood sugar, improving sleep, or correcting deficiencies, ovarian decline is less likely to be the primary cause. Blood tests provide far more clarity than symptom comparison alone.
At what age is perimenopause actually likely to start?
Perimenopause typically begins in the mid to late 40s, although this varies.
While some women experience changes earlier, ovarian decline is not the most likely explanation for symptoms in the late 20s, 30s, or early 40s.
In these age groups, nutrient depletion, chronic stress, under-fuelling, and blood sugar dysregulation are statistically more common causes of fatigue, mood changes, sleep issues, and brain fog.
Should I get blood tests before assuming perimenopause?
Yes, if you want clarity rather than confusion.
Blood tests can identify common deficiencies such as iron, vitamin B12, vitamin D, and markers related to blood sugar regulation.
Testing does not rule out perimenopause forever, but it helps avoid mislabelling symptoms and missing correctable issues. Fixing deficiencies early can also reduce the severity of symptoms later in life.
Can ignoring deficiencies now make perimenopause worse later?
Potentially, yes.
Long-term nutrient depletion, unstable blood sugar, and chronic stress place additional strain on the hormonal system.
While they do not cause perimenopause, they can amplify symptoms when true hormonal transitions occur. Addressing foundational health earlier supports resilience later.
Quick Recap: Perimenopause or Deficiency?
| Symptom | Often assumed to be perimenopause | More commonly linked to | Clue it may not be ovarian decline |
| Fatigue and low energy | Hormonal changes | Iron, B12, vitamin D deficiency, poor sleep, low protein | Energy improves after supplementation or better sleep |
| Brain fog and poor concentration | Hormone imbalance | Iron deficiency, B12 or folate deficiency, blood sugar instability | Worse between meals, better after eating |
| Anxiety or low mood | Perimenopausal anxiety | Magnesium or B6 deficiency, blood sugar crashes, chronic stress | Mood fluctuates daily, not cyclically |
| Sleep problems or night waking | Hormonal night disturbances | Magnesium deficiency, blood sugar dips, caffeine, poor circadian rhythm | Waking at 2–4 am without night sweats |
| Hair thinning or hair loss | Hormonal hair loss | Iron deficiency, low protein, stress, illness | Hair loss follows dieting, stress, or illness |
| Weight gain or difficulty losing weight | “Menopause metabolism” | Insulin resistance, blood sugar dysregulation, stress, low muscle mass | Central weight gain with cravings and crashes |
| Irregular or heavier periods | Perimenopause | Iron deficiency feedback loop, stress, under-fuelling | Cycles stabilise after addressing basics |
| Joint pain or muscle aches | Hormonal decline | Vitamin D or magnesium deficiency, dehydration, inflammation | Pain improves with hydration or supplementation |
| Palpitations or wired-but-tired feeling | Hormonal anxiety | Iron deficiency, magnesium deficiency, caffeine, blood sugar dips | Symptoms track food, stress, or stimulants |
| Feeling “not like yourself” | Early perimenopause | Long-term depletion, burnout, poor recovery, chronic stress | No clear cycle pattern, just constant exhaustion |
The grounded takeaway
Perimenopause content is everywhere, but bodies do not follow trends. Many women in their late 20s, 30s, and early 40s are not experiencing ovarian decline, they are experiencing depletion.
Foundational health is not basic because it is unimportant. Foundational health is basic because it is the base layer, and ignoring it can make future hormonal transitions harder.
Iron Deficiency
McClung, J.P. and Murray-Kolb, L.E. (2013) Iron nutrition and premenopausal women: effects of poor iron status on physical and neuropsychological performance. Annual Review of Nutrition, 33, pp. 271–288. https://pubmed.ncbi.nlm.nih.gov/23642204/
Tardy, A.L., Pouteau, E., Marquez, D., Yilmaz, C. and Scholey, A. (2020) Vitamins and minerals for energy, fatigue and cognition: a narrative review of the biochemical and clinical evidence. Nutrients, 12(1), 228. https://pmc.ncbi.nlm.nih.gov/articles/PMC7019700/
Vitamin B12 and Folate Deficiency
Lachner, C., Steinle, N.I. and Regenold, W.T. (2012) The neuropsychiatry of vitamin B12 deficiency in elderly patients. Journal of Neuropsychiatry and Clinical Neurosciences, 24(1), pp. 5–15. https://pubmed.ncbi.nlm.nih.gov/22450609/
O’Leary, F. and Samman, S. (2010) Vitamin B12 in health and disease. Nutrients, 2(3), pp. 299–316. https://pubmed.ncbi.nlm.nih.gov/22254022/
Vitamin D Deficiency
Eyles, D.W., Burne, T.H.J. and McGrath, J.J. (2013) Vitamin D, effects on brain development, adult brain function and the links between low levels of vitamin D and neuropsychiatric disease. Frontiers in Neuroendocrinology, 34(1), pp. 47–64. https://pubmed.ncbi.nlm.nih.gov/22796576/
Parker, G., Brotchie, H. and Graham, R. (2017) Vitamin D and depression. Journal of Affective Disorders, 208, pp. 56–61. https://pubmed.ncbi.nlm.nih.gov/27750060/
Vitamin B6 (Pyridoxine) Deficiency
Parra, M., Stahl, S. and Hellmann, H. (2018) Vitamin B6 and its role in cell metabolism and physiology. Cells, 7(7), 84. https://pmc.ncbi.nlm.nih.gov/articles/PMC6071262/
Kennedy, D.O. (2016) B vitamins and the brain: mechanisms, dose and efficacy. Nutrients, 8(2), 68. https://pubmed.ncbi.nlm.nih.gov/26828517/
Magnesium Deficiency
de Baaij, J.H.F., Hoenderop, J.G.J. and Bindels, R.J.M. (2015) Magnesium in man: implications for health and disease. Physiological Reviews, 95(1), pp. 1–46. https://pubmed.ncbi.nlm.nih.gov/25540137/
Rosanoff, A., Weaver, C.M. and Rude, R.K. (2012) Suboptimal magnesium status in the United States: are the health consequences underestimated? Nutrition Reviews, 70(3), pp. 153–164. https://pubmed.ncbi.nlm.nih.gov/22364157/
Blood Sugar Dysregulation and Mood or Fatigue
Ludwig, D.S., Ebbeling, C.B. and Holt, S.H.A. (2018) Dietary carbohydrates, blood sugar regulation and metabolic health. BMJ, 361, k2340. https://pmc.ncbi.nlm.nih.gov/articles/PMC5996878/
Benton, D. and Parker, P.Y. (1998) Breakfast, blood glucose, and cognition. American Journal of Clinical Nutrition, 67(4), pp. 772S–778S. https://pubmed.ncbi.nlm.nih.gov/9537627/